Part 2: importance of whole-body movement and specific exercises
Why do we consider other body parts?
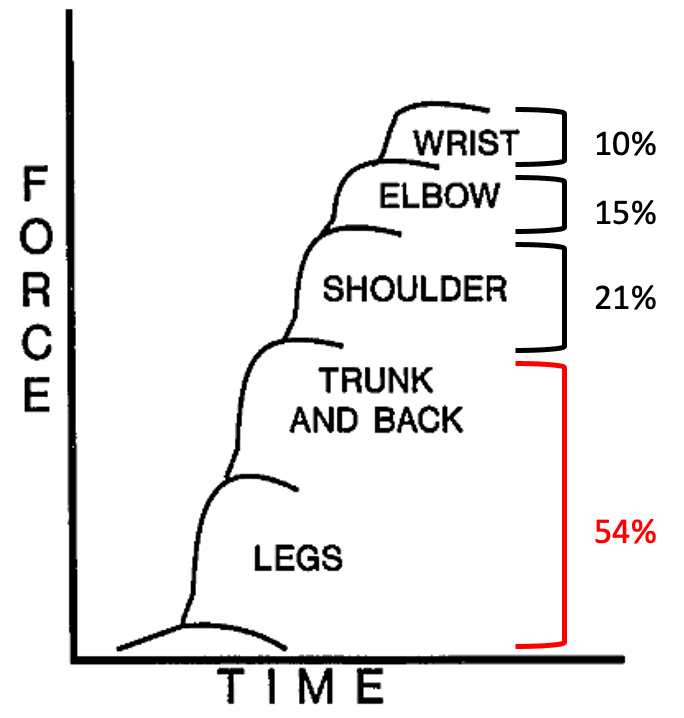
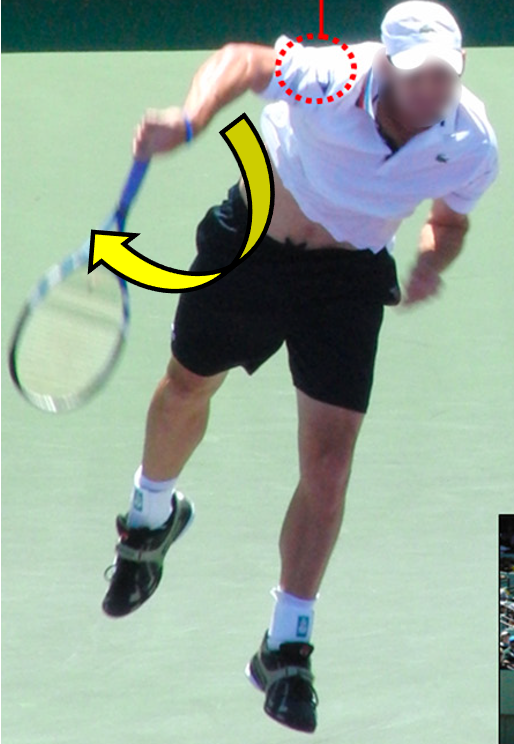
Tennis swing necessitates coordinated movement involving the ankle, knee, hip, trunk, shoulder, elbow, and wrist. Research indicates that over half of the force exerted on the ball during a tennis swing originates from the legs and trunk (54%), followed by the shoulder (21%), elbow (15%), and wrist (10%). Compensatory elbow muscle engagement due to inadequate trunk, leg, and shoulder force production can result in elbow pain despite normal elbow function. I will provide an explanation of how the elbow undergoes significant stress, ultimately leading to the development of tennis elbow.
Image: force production during tennis service
Tennis service
The tennis service motion is composed of several phases. I will discuss specific phases, including the loading, cocking, and deceleration phases. Any weakness or inefficiency in these phases could lead to shoulder or elbow pain.
Loading phase
In the loading phase, the server bends both knees and lowers the shoulder, storing energy transmitted to the arm in subsequent phases. Research reveals that enhanced force production from the legs in this phase boosts service velocity. Calf and quad muscles are key force generators here. Insufficient strength to maintain this position prevents effective use of force from the legs and trunk, necessitating increased shoulder and elbow effort.
Mobility of the spine (backbone) is crucial in this stance. Proper trunk mobility is essential during the loading phase, where the trunk is bent to the right and backward. Inadequate trunk mobility results in excessive shoulder extension, which in turn heightens stress on the shoulder and elbow.
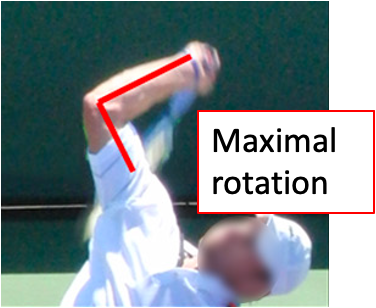
Cocking phase
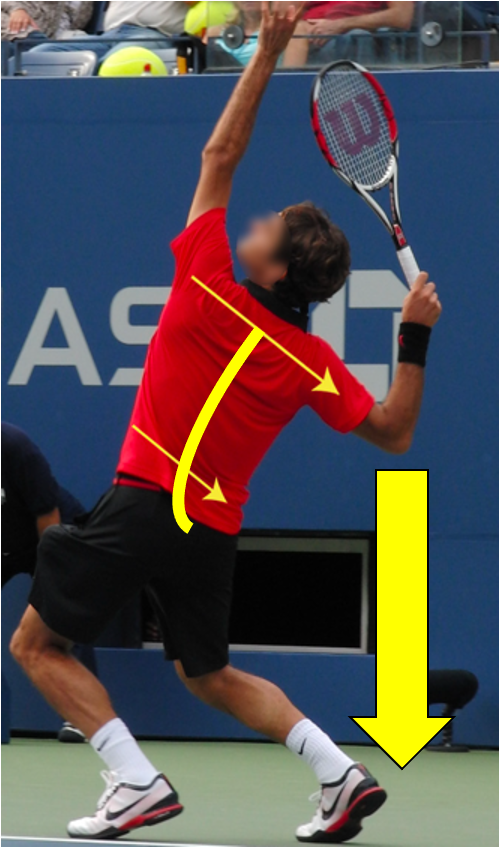
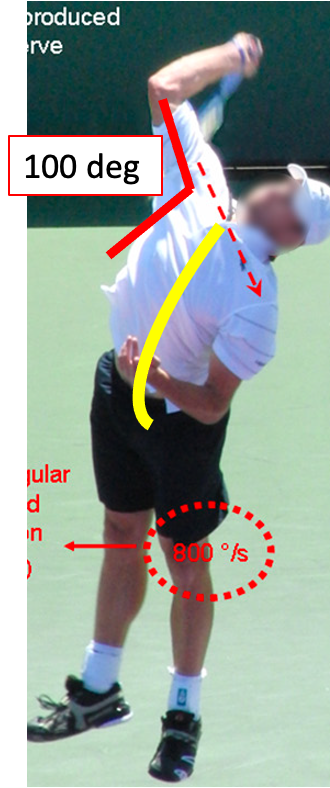
The cocking phase occurs when the shoulder is maximally rotated and stretched. During this phase, both legs should be extended to deliver force to the trunk and shoulder. Hip and trunk muscles then generate left rotational force (obliques, hip adductors, hip flexors, erector spinae). The shoulder is in full external rotation and approximately 100 degrees of abduction, placing stress on the shoulder joint. Shoulder internal rotational strength, produced by subscapularis, latissimus dorsi, and pectoralis major muscles, is necessary for swing acceleration. Inadequate function of these muscles can lead to excessive elbow muscle engagement, potentially causing tennis elbow.
As you see the picture on the left, the server’s trunk leans to the left side, a motion vital for reducing shoulder and elbow stress. Inadequate leftward lean forces the shoulder to open excessively (>100 degrees) to achieve a top hit, placing additional strain on the shoulder. Abnormal shoulder positioning caused from inadequate trunk control elevates the risk of elbow or shoulder pain.
Deceleration phase (follow through)
The deceleration phase involves stopping the swing after hitting the ball. This phase exerts the most stress on arm muscles due to the requirement for eccentric muscle control. After striking the ball, shoulder external rotators are engaged to slow down arm internal rotation and trunk left rotation. Individuals with muscle overuse, including tennis elbow, often experience pain during this phase. Poor eccentric muscle control in the shoulder necessitates excessive elbow usage to decelerate the motion.
Interventions to improve performance
As mentioned earlier, improving leg, trunk, and shoulder performance can reduce elbow stress during tennis. Consult your trainer to determine the necessary training. Some individuals may require hip mobility exercises, while others may benefit from trunk stability and control exercises. The training examples provided below are specific to tennis-related body part training.
Hip mobility exercises
Hip rotation mobility is crucial for generating powerful rotational force during a tennis swing. Mobility exercises are most effective when muscles are engaged at the end of the range of motion. Below are two examples of hip mobility exercises:
- Hip external and internal rotation exercises with Theraband resistance. Ensure that you do not move your pelvis as a compensation instead of the hip joint. If you rotate your back or pelvis, the quality of the exercise will decrease.
- The second exercise is an advanced hip internal rotation exercise because you need to maintain balance during the motion. If you feel that your balance is off during this exercise, you can use a dowel or wall to reduce balance disturbances. Once again, you should not compensate with pelvic or trunk motion due to a lack of hip mobility. Adjust the block height based on your hip mobility.
Hip exercise 1: hip external rotation (clam shell) and internal rotation
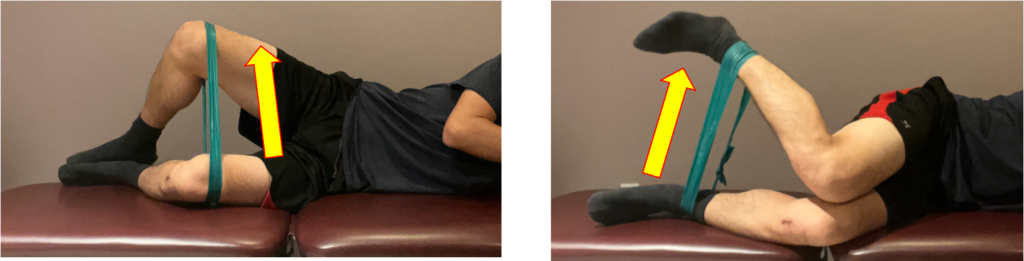
Hip exercise 2: hip internal rotation in kneeling position

Trunk mobility and strengthening exercises
Trunk function is necessary for all movements and postures in our lives, including sitting, walking, running, and the tennis swing. Before attempting the exercises shown below, you should be able to control your trunk inner muscles properly. Ask a physical therapist or trainer to assess whether your trunk muscle function is good enough for trunk strengthening training. If you perform trunk strengthening exercises with poor inner muscle function, you risk injury or a decrease in the quality of your movement.
- Child’s pose to stretch the glutes, latissimus dorsi, and lower back. Once you are in the stretching position, you may repeat the action of gently pushing your arm down into the floor (3 seconds) and then relaxing to improve the flexibility of the latissimus dorsi muscle.
- Trunk rotation with Theraband resistance: Slightly bend your knees and hips to assume a small squat position. Once you feel stable leg support, rotate your arms and trunk while maintaining a stable pelvis. Keep your pelvis facing forward during the motion. Start with light resistance (yellow or red-colored band), then progress to a stronger band (green, blue) as you can easily complete 3 sets of 10 repetitions. Adjust the band’s height to different levels because you need to swing at various heights during a tennis match. Additionally, incorporate quick rotations with light weights into your routine as your muscles need to engage at high velocity during a tennis swing.
Trunk mobility exercise: child pose

Trunk strengthening exercise: Theraband (or cable) rotation in different angle

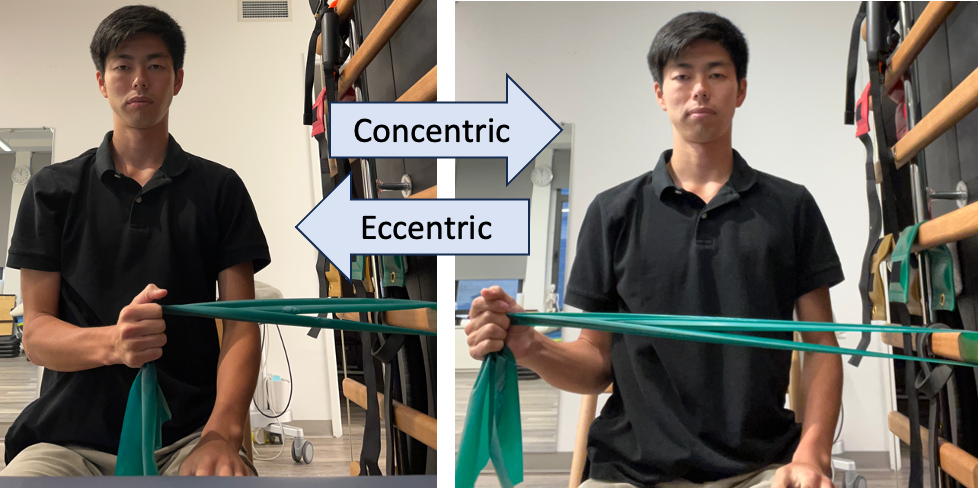
Shoulder concentric and eccentric rotation training
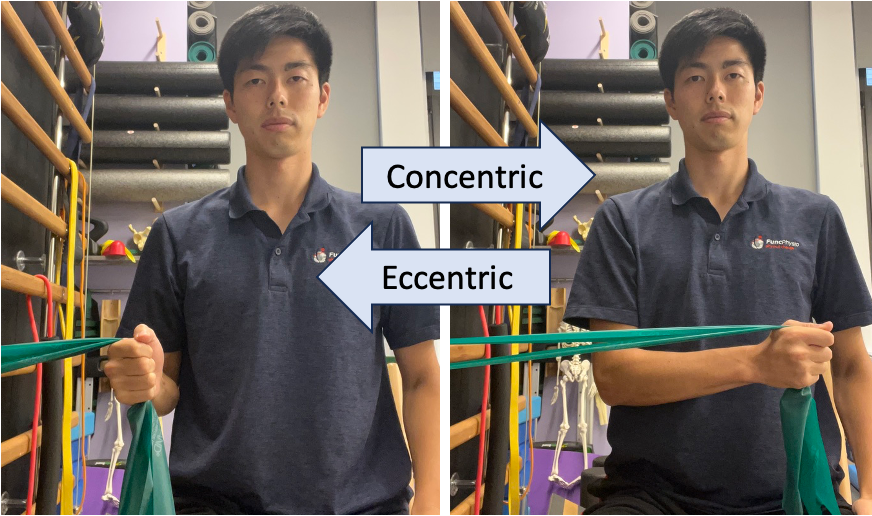
As I mentioned earlier, shoulder muscles are under the most stress during the deceleration phase with eccentric contraction. Tennis players often experience back problems because they compensate for a lack of shoulder rotation strength with trunk rotation. Shoulder muscles need to be engaged both concentrically (muscle fibers shortened) and eccentrically (muscle fibers lengthened).
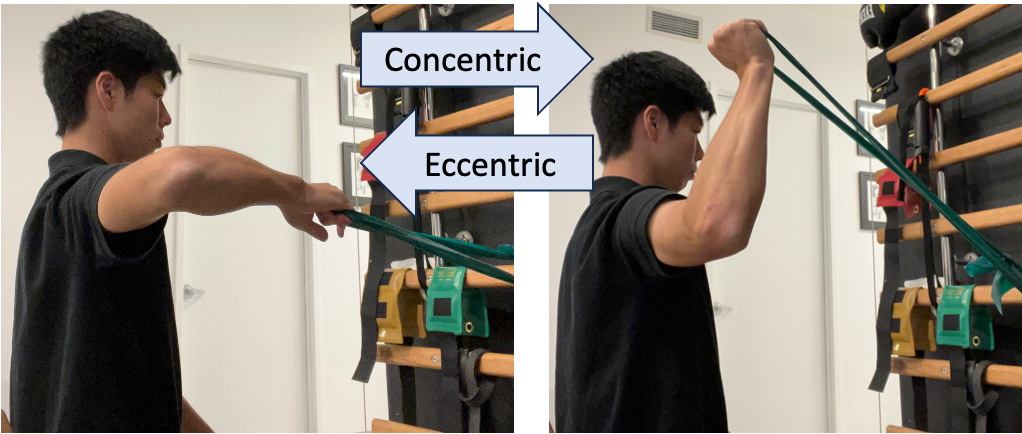
During serving and forehand swings, shoulder internal rotators are engaged concentrically, and external rotators eccentrically. On the other hand, during a backhand swing, shoulder external rotators are engaged concentrically, and internal rotators eccentrically. Therefore, you need to practice both directions of internal and external shoulder rotation, both concentrically and eccentrically. To train eccentric control specifically, you can slowly return to the initial position while the muscle is engaged. You may practice in two different shoulder positions to
Internal rotation exercise
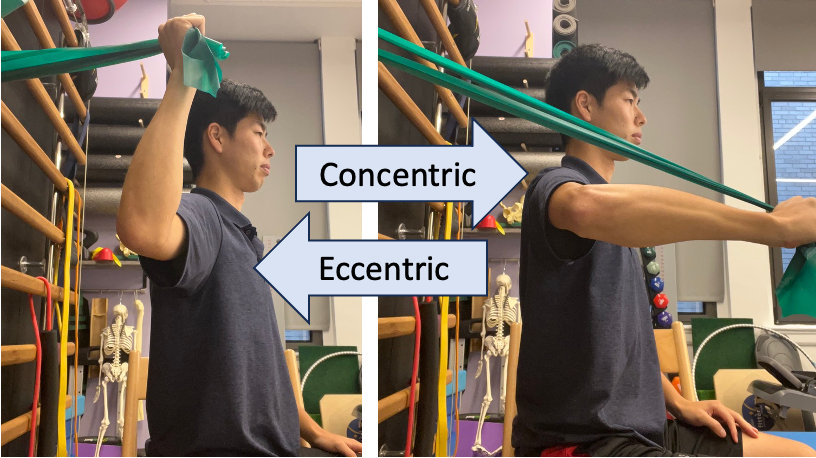
External rotation exercise
Conclusion
I hope you have gained a better understanding of how physical therapists treat tennis elbow. I discussed tennis elbow in my last two blogs. In part one, I covered the diagnosis and treatment plans for tennis elbow, and in part two, I introduced specific exercises to improve your tennis swing.
In reality, it can be challenging to identify your own physical problems. You can often determine the appropriate treatment or exercises with an assessment performed by a physical therapist or a trainer. Please don’t hesitate to consult professionals to enhance your performance. Thank you for reading!
Reference
1: Bhabra, G., Wang, A., Ebert, JR., et al. Lateral Elbow Tendinopathy: Development of a Pathophysiology-Based Treatment Algorithm. Orthop J Sports Med. 2016 Nov 1;4(11).
2. Lucado, AM., Day, JM., Vincent, JI., et al. Lateral Elbow Pain and Muscle Function Impairments. J Orthop Sports Phys Ther. 2022 Dec;52(12).
3. Obuchowicz, R., Bonczar, M. Ultrasonographic Differentiation of Lateral Elbow Pain. Ultrasound Int Open. 2016 May;2(2):E38-46.
4. Kovacs, M., Ellenbecker, T. An 8-stage model for evaluating the tennis serve: implications for performance enhancement and injury prevention. Sports Health. 2011 Nov;3(6):504-13.


